Business Name: BeeHive Homes Assisted Living
Address: 16220 West Rd, Houston, TX 77095
Phone: (832) 906-6460
BeeHive Homes Assisted Living
BeeHive Homes Assisted Living of Cypress offers assisted living and memory care services in a warm, comfortable, and residential setting. Our care philosophy focuses on personalized support, safety, dignity, and building meaningful connections for each resident. Welcoming new residents from the Cypress and surrounding Houston TX community.
16220 West Rd, Houston, TX 77095
Business Hours
Monday thru Sunday: 7:00am - 7:00pm
Facebook: https://www.facebook.com/BeeHiveHomesCypress
Senior care has been developing from a set of siloed services into a continuum that meets people where they are. The old model asked families to select a lane, then change lanes abruptly when requires altered. The more recent method blends assisted living, memory care, and respite care, so that a resident can move supports without losing familiar faces, regimens, or self-respect. Designing that type of incorporated experience takes more than good intents. It requires careful staffing designs, clinical protocols, constructing style, data discipline, and a desire to reassess charge structures.
I have actually walked families through intake interviews where Dad insists he still drives, Mom says she is great, and their adult kids look at the scuffed bumper and silently inquire about nighttime roaming. Because meeting, you see why strict categories fail. People seldom fit neat labels. Requirements overlap, wax, and wane. The better we mix services across assisted living and memory care, and weave respite care in for stability, the most likely we are to keep homeowners safer and families sane.
The case for blending services instead of splitting them
Assisted living, memory care, and respite care established along different tracks for strong reasons. Assisted living centers concentrated on assist with activities of daily living, medication support, meals, and social programs. Memory care systems built specialized environments and training for homeowners with cognitive impairment. Respite care produced brief stays so family caregivers might rest or manage a crisis. The separation worked when communities were smaller and the population simpler. It works less well now, with increasing rates of mild cognitive problems, multimorbidity, and household caregivers stretched thin.
Blending services unlocks a number of benefits. Homeowners prevent unnecessary moves when a new symptom appears. Employee are familiar with the individual over time, not simply a diagnosis. Families get a single point of contact and a steadier plan for financial resources, which reduces the psychological turbulence that follows abrupt transitions. Communities also gain operational flexibility. Throughout flu season, for instance, a system with more nurse protection can bend to handle greater medication administration or increased monitoring.
All of that features compromises. Combined designs can blur scientific requirements and welcome scope creep. Personnel might feel uncertain about when to intensify from a lighter-touch assisted living setting to memory care level procedures. If respite care ends up being the safety valve for every gap, schedules get untidy and tenancy planning becomes guesswork. It takes disciplined admission criteria, regular reassessment, and clear internal communication to make the mixed method humane instead of chaotic.
What mixing appears like on the ground
The finest integrated programs make the lines permeable without pretending there are no differences. I like to think in 3 layers.
First, a shared core. Dining, house cleaning, activities, and upkeep needs to feel smooth throughout assisted living and memory care. Locals belong to the entire community. Individuals with cognitive changes still delight in the noise of the piano at lunch, or the feel of soil in a gardening club, if the setting is attentively adapted.
Second, tailored procedures. Medication management in assisted living may operate on a four-hour pass cycle with eMAR verification and spot vitals. In memory care, you include regular discomfort assessment for nonverbal hints and a smaller sized dosage of PRN psychotropics with tighter review. Respite care includes consumption screenings created to record an unfamiliar person's baseline, since a three-day stay leaves little time to discover the typical habits pattern.
Third, ecological cues. Combined neighborhoods purchase style that preserves autonomy while preventing damage. Contrasting toilet seats, lever door deals with, circadian lighting, peaceful areas anywhere the ambient level runs high, and wayfinding landmarks that do not infantilize. I have seen a corridor mural of a regional lake transform evening pacing. Individuals stopped at the "water," talked, and returned to a lounge rather of heading for an exit.
Intake and reassessment: the engine of a blended model
Good consumption prevents lots of downstream issues. A thorough consumption for a blended program looks various from a basic assisted living questionnaire. Beyond ADLs and medication lists, we need details on regimens, personal triggers, food preferences, movement patterns, wandering history, urinary health, and any hospitalizations in the previous year. Families frequently hold the most nuanced information, however they may underreport habits from humiliation or overreport from fear. I ask particular, nonjudgmental concerns: Has there been a time in the last month when your mom woke in the evening and attempted to leave the home? If yes, what occurred right before? Did caffeine or late-evening TV play a role? How often?
Reassessment is the second important piece. In integrated neighborhoods, I favor a 30-60-90 day cadence after move-in, then quarterly unless there is a modification of condition. Shorter checks follow any ED visit or new medication. Memory changes are subtle. A resident who used to navigate to breakfast may start hovering at an entrance. That could be the first indication of spatial disorientation. In a mixed design, the group can nudge supports up carefully: color contrast on door frames, a volunteer guide for the early morning hour, extra signs at eye level. If those modifications stop working, the care plan intensifies instead of the resident being uprooted.

Staffing designs that in fact work
Blending services works just if staffing expects variability. The typical mistake is to staff assisted living lean and then "borrow" from memory care during rough patches. That erodes both sides. I choose a staffing matrix that sets a base ratio for each program and designates float capability throughout a geographic zone, not unit lines. On a common weekday in a 90-resident community with 30 in memory care, you might see one nurse for each program, care partners at 1 to 8 in assisted living during peak early morning hours, 1 to 6 in memory care, and an activities group that staggers start times to match behavioral patterns. A devoted medication specialist can minimize mistake rates, however cross-training a care partner as a backup is essential for ill calls.
Training should exceed the minimums. State guidelines often require only a few hours of dementia training every year. That is not enough. Efficient programs run scenario-based drills. Personnel practice de-escalation for sundowning, redirection during exit looking for, and safe transfers with resistance. Supervisors must shadow brand-new hires across both assisted living and memory care for a minimum of 2 full shifts, and respite employee need a tighter orientation on quick relationship structure, because they might have only days with the guest.
Another overlooked element is personnel psychological assistance. Burnout hits quick when groups feel obligated to be everything to everyone. Arranged huddles matter: 10 minutes at 2 p.m. to sign in on who requires a break, which locals need eyes-on, and whether anyone is bring a heavy interaction. A brief reset can avoid a medication pass error or a frayed reaction to a distressed resident.
Technology worth using, and what to skip
Technology can extend personnel capabilities if it is easy, consistent, and tied to outcomes. In combined communities, I have actually discovered 4 classifications helpful.
Electronic care planning and eMAR systems reduce transcription mistakes and develop a record you can trend. If a resident's PRN anxiolytic use climbs up from two times a week to daily, the system can flag it for the nurse in charge, triggering an origin check before a behavior ends up being entrenched.
Wander management requires careful implementation. Door alarms are blunt instruments. Much better choices consist of discreet wearable tags connected to specific exit points or a virtual limit that alerts personnel when a resident nears a threat zone. The goal is to avoid a lockdown feel while preventing elopement. Households accept these systems quicker when they see them coupled with meaningful activity, not as a substitute for engagement.
Sensor-based tracking can add value for fall threat and sleep tracking. Bed sensing units that discover weight shifts and notify after a pre-programmed stillness interval assistance staff step in with toileting or repositioning. But you need to calibrate the alert limit. Too delicate, and staff ignore the sound. Too dull, and you miss real risk. Little pilots are crucial.
Communication tools for families minimize anxiety and phone tag. A secure app that posts a quick note and a picture from the early morning activity keeps relatives informed, and you can use it to arrange care conferences. Avoid apps that include complexity or require staff to bring multiple gadgets. If the system does not incorporate with your care platform, it will die under the weight of double documentation.
I am wary of innovations that assure to infer state of mind from facial analysis or predict elderly care agitation without context. Teams begin to trust the control panel over their own observations, and interventions wander generic. The human work still matters most: understanding that Mrs. C begins humming before she attempts to load, or that Mr. R's pacing slows with a hand massage and Sinatra.
Program style that respects both autonomy and safety
The most basic method to undermine integration is to cover every safety measure in restriction. Citizens know when they are being corralled. Dignity fractures rapidly. Excellent programs choose friction where it helps and eliminate friction where it harms.
Dining shows the compromises. Some neighborhoods isolate memory care mealtimes to control stimuli. Others bring everybody into a single dining room and produce smaller "tables within the space" using layout and seating plans. The second method tends to increase hunger and social cues, however it requires more personnel flow and clever acoustics. I have had success pairing a quieter corner with material panels and indirect lighting, with an employee stationed for cueing. For residents with dyspagia, we serve modified textures attractively instead of defaulting to dull purees. When households see their loved ones enjoy food, they begin to trust the mixed setting.
Activity shows should be layered. A morning chair yoga group can cover both assisted living and memory care if the instructor adapts hints. Later on, a smaller cognitive stimulation session may be used only to those who benefit, with customized jobs like arranging postcards by decade or assembling simple wood packages. Music is the universal solvent. The ideal playlist can knit a room together quick. Keep instruments available for spontaneous usage, not secured a closet for set up times.
Outdoor access deserves top priority. A secure yard linked to both assisted living and memory care doubles as a tranquil space for respite visitors to decompress. Raised beds, wide paths without dead ends, and a location to sit every 30 to 40 feet invite usage. The capability to wander and feel the breeze is not a luxury. It is often the difference in between a calm afternoon and a behavioral spiral.
Respite care as stabilizer and on-ramp
Respite care gets treated as an afterthought in numerous communities. In incorporated designs, it is a strategic tool. Families require a break, definitely, however the worth surpasses rest. A well-run respite program functions as a pressure release when a caretaker is nearing burnout. It is a trial stay that exposes how an individual responds to new regimens, medications, or ecological hints. It is also a bridge after a hospitalization, when home may be unsafe for a week or two.
To make respite care work, admissions need to be quick but not cursory. I go for a 24 to 72 hour turn time from inquiry to move-in. That needs a standing block of provided spaces and a pre-packed consumption kit that personnel can resolve. The package consists of a brief standard form, medication reconciliation checklist, fall risk screen, and a cultural and individual choice sheet. Households must be welcomed to leave a few concrete memory anchors: a favorite blanket, photos, a scent the person connects with comfort. After the very first 24 hours, the team needs to call the family proactively with a status upgrade. That phone call develops trust and typically reveals an information the intake missed.
Length of stay varies. Three to seven days is common. Some neighborhoods offer up to 30 days if state policies permit and the individual fulfills criteria. Prices must be transparent. Flat per-diem rates reduce confusion, and it helps to bundle the fundamentals: meals, day-to-day activities, standard medication passes. Additional nursing needs can be add-ons, however prevent nickel-and-diming for ordinary assistances. After the stay, a brief composed summary assists households understand what worked out and what might need adjusting at home. Numerous eventually transform to full-time residency with much less fear, given that they have actually currently seen the environment and the staff in action.
Pricing and transparency that households can trust
Families dread the financial maze as much as they fear the relocation itself. Mixed models can either clarify or make complex costs. The much better approach utilizes a base rate for home size and a tiered care plan that is reassessed at predictable intervals. If a resident shifts from assisted living to memory care level supports, the increase should show real resource usage: staffing strength, specialized programming, and medical oversight. Prevent surprise fees for routine behaviors like cueing or accompanying to meals. Build those into tiers.
It assists to share the math. If the memory care supplement funds 24-hour protected access points, greater direct care ratios, and a program director concentrated on cognitive health, say so. When households understand what they are buying, they accept the cost quicker. For respite care, publish the day-to-day rate and what it includes. Deal a deposit policy that is fair however firm, given that last-minute changes stress staffing.
Veterans advantages, long-term care insurance coverage, and Medicaid waivers vary by state. Staff should be proficient in the basics and understand when to refer families to an advantages specialist. A five-minute discussion about Help and Participation can alter whether a couple feels required to offer a home quickly.
When not to mix: guardrails and red lines
Integrated designs should not be an excuse to keep everyone all over. Security and quality dictate certain red lines. A resident with consistent aggressive behavior that hurts others can not stay in a general assisted living environment, even with extra staffing, unless the habits stabilizes. A person requiring constant two-person transfers may exceed what a memory care unit can securely provide, depending upon layout and staffing. Tube feeding, complex injury care with day-to-day dressing modifications, and IV therapy often belong in a proficient nursing setting or with contracted scientific services that some assisted living neighborhoods can not support.
There are likewise times when a completely protected memory care neighborhood is the ideal call from day one. Clear patterns of elopement intent, disorientation that does not respond to environmental hints, or high-risk comorbidities like unrestrained diabetes paired with cognitive impairment warrant caution. The secret is honest evaluation and a desire to refer out when suitable. Homeowners and families remember the stability of that choice long after the instant crisis passes.
Quality metrics you can in fact track
If a neighborhood declares mixed quality, it ought to show it. The metrics do not require to be fancy, but they must be consistent.
- Staff-to-resident ratios by shift and by program, published month-to-month to leadership and reviewed with staff. Medication error rate, with near-miss tracking, and an easy corrective action loop. Falls per 1,000 resident days, separated by assisted living and memory care, and an evaluation of falls within 1 month of move-in or level-of-care change. Hospital transfers and return-to-hospital within 30 days, keeping in mind avoidable causes. Family satisfaction ratings from short quarterly surveys with two open-ended questions.
Tie rewards to improvements homeowners can feel, not vanity metrics. For example, lowering night-time falls after changing lighting and evening activity is a win. Announce what changed. Personnel take pride when they see information show their efforts.
Designing buildings that flex rather than fragment
Architecture either helps or combats care. In a mixed design, it needs to bend. Systems near high-traffic hubs tend to work well for homeowners who grow on stimulation. Quieter homes permit decompression. Sight lines matter. If a group can not see the length of a corridor, action times lag. Wider passages with seating nooks turn aimless walking into purposeful pauses.
Doors can be threats or invites. Standardizing lever deals with assists arthritic hands. Contrasting colors in between flooring and wall ease depth understanding concerns. Prevent patterned carpets that appear like actions or holes to somebody with visual processing difficulties. Kitchens benefit from partial open designs so cooking aromas reach communal spaces and promote cravings, while devices stay securely inaccessible to those at risk.
Creating "porous limits" between assisted living and memory care can be as easy as shared courtyards and program rooms with set up crossover times. Put the beauty parlor and therapy fitness center at the seam so citizens from both sides socialize naturally. Keep personnel break rooms main to encourage quick partnership, not stashed at the end of a maze.
Partnerships that reinforce the model
No neighborhood is an island. Primary care groups that devote to on-site check outs reduced transportation turmoil and missed out on appointments. A visiting pharmacist examining anticholinergic concern once a quarter can lower delirium and falls. Hospice providers who incorporate early with palliative consults prevent roller-coaster medical facility journeys in the last months of life.

Local companies matter as much as medical partners. High school music programs, faith groups, and garden clubs bring intergenerational energy. A neighboring university might run an occupational therapy lab on site. These collaborations expand the circle of normalcy. Homeowners do not feel parked at the edge of town. They stay residents of a living community.
Real households, genuine pivots
One family lastly gave in to respite care after a year of nighttime caregiving. Their mother, a former instructor with early Alzheimer's, arrived doubtful. She slept ten hours the opening night. On day two, she remedied a volunteer's grammar with pleasure and joined a book circle the team customized to narratives rather than books. That week revealed her capacity for structured social time and her trouble around 5 p.m. The household moved her in a month later, currently relying on the personnel who had discovered her sweet spot was midmorning and scheduled her showers then.
Another case went the other method. A retired mechanic with Parkinson's and mild cognitive changes wanted assisted living near his garage. He loved pals at lunch but started roaming into storage areas by late afternoon. The team tried visual cues and a walking club. After 2 minor elopement efforts, the nurse led a family conference. They agreed on a move into the protected memory care wing, keeping his afternoon job time with an employee and a small bench in the courtyard. The wandering stopped. He gained two pounds and smiled more. The blended program did not keep him in place at all costs. It helped him land where he could be both free and safe.
What leaders must do next
If you run a neighborhood and wish to mix services, begin with three relocations. Initially, map your present resident journeys, from inquiry to move-out, and mark the points where individuals stumble. That shows where combination can assist. Second, pilot a couple of cross-program elements instead of rewriting everything. For instance, merge activity calendars for 2 afternoon hours and add a shared staff huddle. Third, clean up your data. Choose five metrics, track them, and share the trendline with personnel and families.
Families evaluating neighborhoods can ask a couple of pointed concerns. How do you choose when somebody requires memory care level support? What will change in the care strategy before you move my mother? Can we set up respite remain in advance, and what would you want from us to make those successful? How frequently do you reassess, and who will call me if something shifts? The quality of the answers speaks volumes about whether the culture is really integrated or simply marketed that way.
The guarantee of mixed assisted living, memory care, and respite care is not that we can stop decline or eliminate difficult options. The pledge is steadier ground. Regimens that endure a bad week. Spaces that feel like home even when the mind misfires. Staff who know the person behind the medical diagnosis and have the tools to act. When we build that sort of environment, the labels matter less. The life in between them matters more.
BeeHive Homes Assisted Living is an Assisted Living Facility
BeeHive Homes Assisted Living is an Assisted Living Home
BeeHive Homes Assisted Living is located in Cypress, Texas
BeeHive Homes Assisted Living is located Northwest Houston, Texas
BeeHive Homes Assisted Living offers Memory Care Services
BeeHive Homes Assisted Living offers Respite Care (short-term stays)
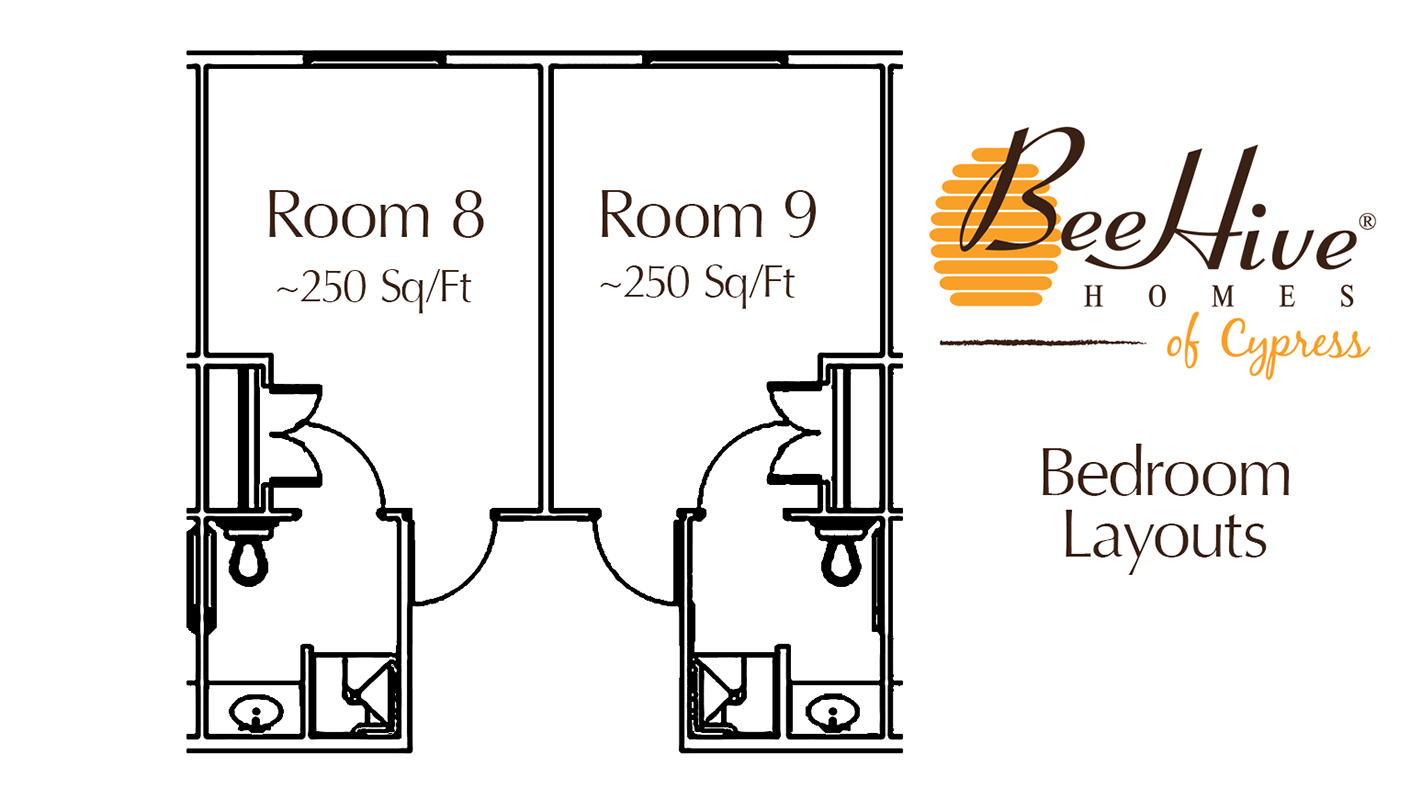
BeeHive Homes Assisted Living provides Private Bedrooms with Private Bathrooms for their senior residents
BeeHive Homes Assisted Living provides 24-Hour Staffing
BeeHive Homes Assisted Living serves Seniors needing Assistance with Activities of Daily Living
BeeHive Homes Assisted Living includes Home-Cooked Meals Dietitian-Approved
BeeHive Homes Assisted Living includes Daily Housekeeping & Laundry Services
BeeHive Homes Assisted Living features Private Garden and Green House
BeeHive Homes Assisted Living has a Hair/Nail Salon on-site
BeeHive Homes Assisted Living has a phone number of (832) 906-6460
BeeHive Homes Assisted Living has an address of 16220 West Road, Houston, TX 77095
BeeHive Homes Assisted Living has website https://beehivehomes.com/locations/cypress
BeeHive Homes Assisted Living has Google Maps listing https://maps.app.goo.gl/G6LUPpVYiH79GEtf8
BeeHive Homes Assisted Living has Facebook page https://www.facebook.com/BeeHiveHomesCypress
BeeHive Homes Assisted Living is part of the brand BeeHive Homes
BeeHive Homes Assisted Living focuses on Smaller, Home-Style Senior Residential Setting
BeeHive Homes Assisted Living has care philosophy of “The Next Best Place to Home”
BeeHive Homes Assisted Living has floorplan of 16 Private Bedrooms with ADA-Compliant Bathrooms
BeeHive Homes Assisted Living welcomes Families for Tours & Consultations
BeeHive Homes Assisted Living promotes Engaging Activities for Senior Residents
BeeHive Homes Assisted Living emphasizes Personalized Care Plans for each Resident
BeeHive Homes Assisted Living won Top Branded Assisted Living Houston 2025
BeeHive Homes Assisted Living earned Outstanding Customer Service Award 2024
BeeHive Homes Assisted Living won Excellence in Assisted Living Homes 2023
People Also Ask about BeeHive Homes Assisted Living
What services does BeeHive Homes Assisted Living of Cypress provide?
BeeHive Homes Assisted Living of Cypress provides a full range of assisted living and memory care services tailored to the needs of seniors. Residents receive help with daily activities such as bathing, dressing, grooming, medication management, and mobility support. The community also offers home-cooked meals, housekeeping, laundry services, and engaging daily activities designed to promote social interaction and cognitive stimulation. For individuals needing specialized support, the secure memory care environment provides additional safety and supervision.
How is BeeHive Homes Assisted Living of Cypress different from larger assisted living facilities?
BeeHive Homes Assisted Living of Cypress stands out for its small-home model, offering a more intimate and personalized environment compared to larger assisted living facilities. With 16 residents, caregivers develop deeper relationships with each individual, leading to personalized attention and higher consistency of care. This residential setting feels more like a real home than a large institution, creating a warm, comfortable atmosphere that helps seniors feel safe, connected, and truly cared for.
Does BeeHive Homes Assisted Living of Cypress offer private rooms?
Yes, BeeHive Homes Assisted Living of Cypress offers private bedrooms with private or ADA-accessible bathrooms for every resident. These rooms allow individuals to maintain dignity, independence, and personal comfort while still having 24-hour access to caregiver support. Private rooms help create a calmer environment, reduce stress for residents with memory challenges, and allow families to personalize the space with familiar belongings to create a “home-within-a-home” feeling.
Where is BeeHive Homes Assisted Living located?
BeeHive Homes Assisted Living is conveniently located at 16220 West Road, Houston, TX 77095. You can easily find direction on Google Maps or visit their home during business hours, Monday through Sunday from 7am to 7pm.
How can I contact BeeHive Homes Assisted Living?
You can contact BeeHive Assisted Living by phone at: 832-906-6460, visit their website at https://beehivehomes.com/locations/cypress, or connect on social media via Facebook
We are near Houston Premium Outlets, easy and close shopping while visiting mom in our assisted living home.